
If you searched for "TSDV vs RBQM" expecting a head-to-head, here's the short version. There isn't one. Targeted source data verification (TSDV) is a verification practice. Risk-based quality management (RBQM) is the wider quality framework. Targeted SDV sits inside RBQM. They work at different levels, so treating them as competing options gets the relationship wrong from the start. The more useful question is how they fit, and that's what the rest of this guide covers.
So why does the comparison keep coming up? Mostly because teams are under real pressure to cut the cost and burden of source data verification, and once monitoring shifts to a risk-based model, it's not obvious where SDV is supposed to land. People reach for "TSDV vs RBQM" because they're trying to work out whether targeted SDV replaces their monitoring strategy, slots into it, or makes a separate platform unnecessary.
Here's the takeaway before the detail. You need a risk-based approach. Within that approach, you want targeted rather than 100% verification, because checking every data point is no longer expected by regulators and rarely earns its keep. The real decision is not whether to target. It's how.
TSDV vs RBQM at a glance
| Targeted SDV (TSDV) | RBQM | |
|---|---|---|
| What it is | Verifying selected source data against the records, rather than all of it | A framework for managing trial quality based on risk |
| Scope | One activity: source data verification | The whole quality and monitoring approach across a trial |
| Problem it solves | Too much monitor time spent verifying low-risk data | Quality risks spread unevenly across sites, data, and processes |
| Where it sits | A component inside a risk-based approach | The level above, holding the components together |
| Regulatory basis | FDA risk-based monitoring guidance (2013); accepted under ICH E6(R3) | ICH E6(R3) treats risk-based quality management as a core expectation |
| Typical tooling | Built into the EDC, or a manual SDV plan | Dedicated centralized monitoring platforms, plus EDC and other systems |
What is targeted source data verification (TSDV)?
Targeted source data verification is the practice of checking a selected subset of source data against the records, instead of verifying everything. You decide what gets verified based on risk, and you leave the rest.
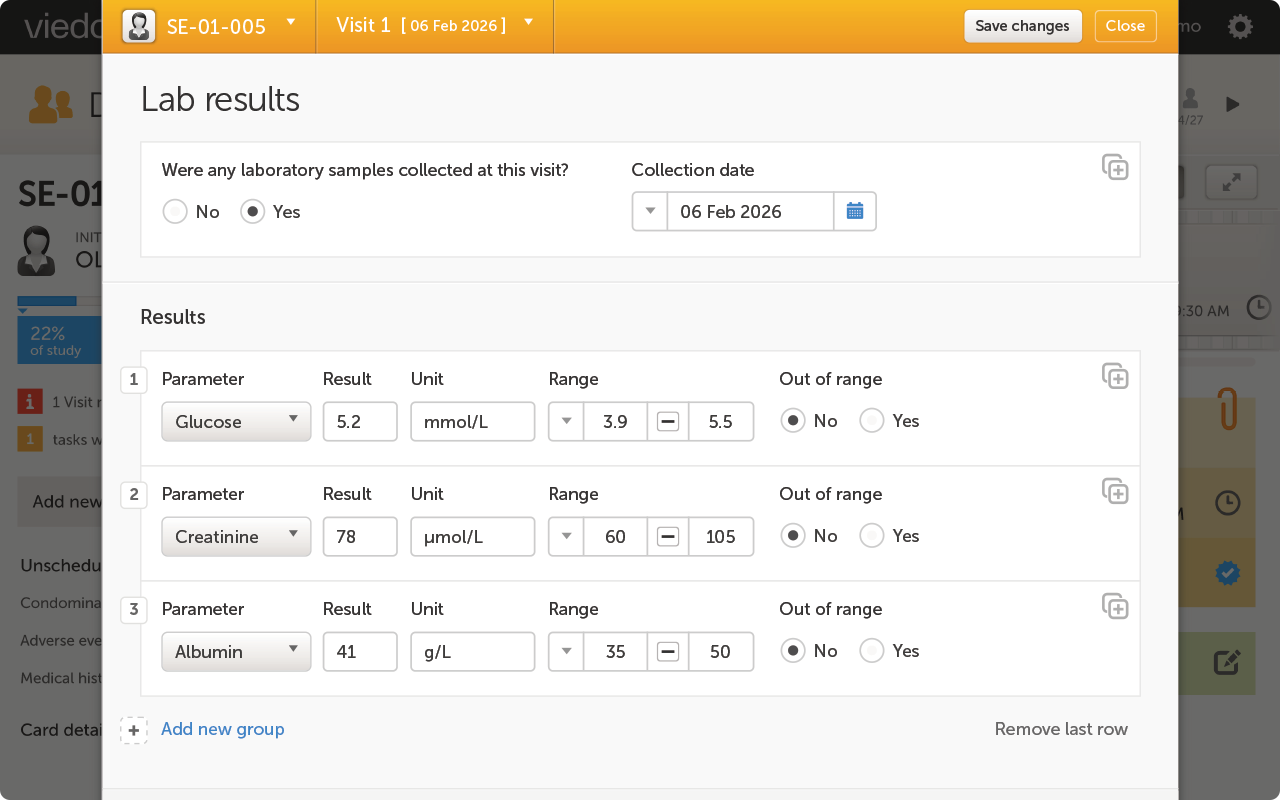
It helps to separate two activities that often get blurred. SDV is verification, confirming that the data in the system matches the source. Source data review (SDR) is different. SDR is the review of the source data itself for completeness, plausibility, and protocol compliance. One checks that the data was transcribed correctly. The other checks that the underlying data makes sense. Targeted SDV is about the first of these, though both belong in a risk-based approach.
There's a further choice inside targeted SDV, and it matters more than most teams expect. You can target by patient, picking a percentage of subjects to verify in full. Or you can target by time period, verifying the data generated in specific windows across all subjects at a site. Hold that distinction. It's the hinge the later sections turn on.
Regulators support this direction. The FDA's 2013 risk-based monitoring guidance accepts targeted SDV, and ICH E6(R3) frames quality management around risk rather than blanket verification. Targeted SDV is no longer the exception. It's the expected way to work.
What is risk-based monitoring (RBM) and risk-based quality management (RBQM)?
Risk-based monitoring (RBM) is the philosophy of directing monitoring effort to where the risk is highest, instead of treating every site, every patient, and every data point the same. The idea is simple. Some data carries more risk than other data, so your attention should follow the risk.
Risk-based quality management (RBQM) is broader. It takes that philosophy and builds a whole framework around it. RBQM adds centralized statistical monitoring, key risk indicator (KRI) tracking, quality tolerance limits, and site risk scoring across the trial. It's the structure that decides where risk lives and how you respond to it, from study design through to closeout.
ICH E6(R3), finalized in 2025, treats risk-based quality management as a core part of good clinical practice. It doesn't prescribe blanket verification, and it doesn't tell you which tools to buy. Dedicated centralized monitoring platforms can carry a lot of the RBQM load, but the framework itself is bigger than any single product.
How TSDV and RBQM fit together
Picture three levels, stacked. At the top sits RBM, the philosophy of focusing on risk. In the middle sits RBQM, the machinery that puts the philosophy to work. Near the ground sits targeted SDV, a specific thing you do to verify data efficiently. Asking "TSDV vs RBQM" is a bit like asking "engine vs car." One is part of the other.
That gives you a clear rule of thumb on dependency. You can run targeted SDV without a full RBQM program. Plenty of teams do, especially on simpler trials where a heavy centralized monitoring setup would be overkill. But you can't really run RBQM without some form of targeted, non-100%, verification. A framework built on focusing effort by risk falls apart if you still verify every data point by hand. Targeted SDV is the part of RBQM that makes the verification side honest.
Now the part that changes how you should target. Site risk tends to cluster in time periods, not in specific patients. Think about what actually goes wrong at a site. New staff arrive and haven't found their feet. A training session gets missed. A protocol amendment lands and the site adjusts. None of these problems pick out individual patients. They affect everyone seen at that site during that window. So if you sample by patient, you can verify a "clean" subject in full and miss the messy fortnight that touched everyone else. Targeting by time period matches where the risk really sits.
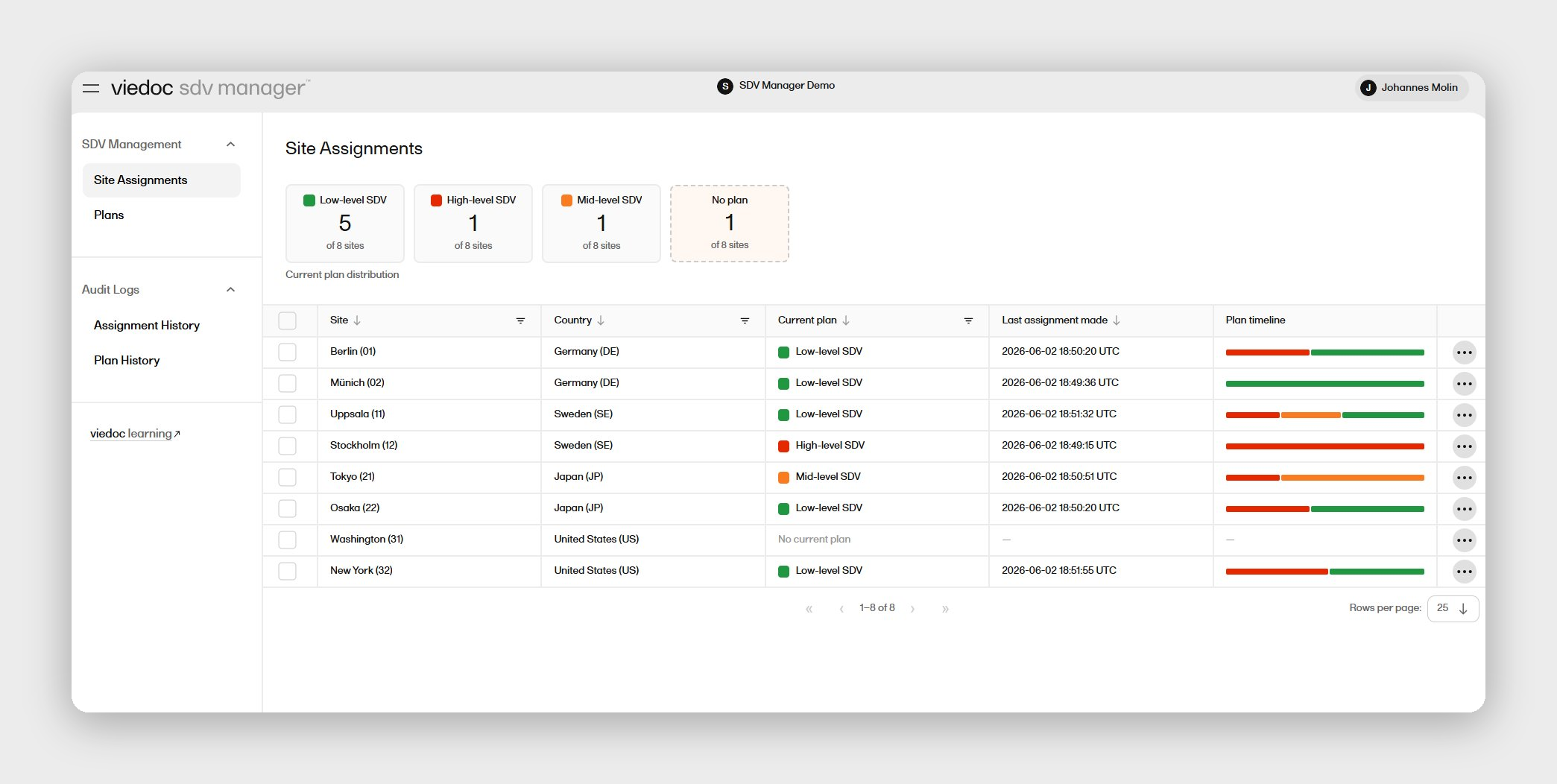
This is where targeted SDV tooling comes in, as the verification component of your approach, not as the framework itself. Viedoc's EDC platform handles this directly through its SDV Manager application, assigning SDV plans by time period rather than by patient. Other platforms target by patient, field, form, or site.
Whether you also need a separate RBQM platform depends on how complex your trial is and how you monitor. A large, multi-region study with heavy centralized statistical monitoring may well want a dedicated platform, and these platforms do that job well. A leaner study, where the main goal is controlling SDV volume sensibly, may not need one. If your risk-based effort is mostly about verifying the right data rather than running KRIs and tolerance limits across dozens of sites, a capable targeted SDV setup inside your EDC software may cover what you need. The point is to match the tooling to the monitoring your trial calls for.
How to apply targeted SDV in your trial
A practical way to put this into action, in five steps.
Step 1: Assess your current SDV burden. Look at how much monitor time goes into verification, and where it lands. If your CRAs are verifying low-risk data at quiet sites with the same intensity as high-risk data at struggling ones, you've found your savings.
Step 2: Decide whether you need full RBQM or risk-based SDV control. Be honest about trial complexity. If you need centralized statistical monitoring, KRIs, and tolerance limits across many sites, you're in RBQM-platform territory. If the core problem is verification volume, you may only need targeted SDV inside your EDC.
Step 3: Define your targets. Ensure SDV plans can be configured for the scenarios you need; where the risk is low and another for when risk is high. Confirming that plans can be assigned to sites in a way to match site risk levels is critical in a risk-based approach to SDV.
Step 4: Confirm audit and inspection readiness. You want to show an inspector an active plan and a clean record: what was verified, when, and by whom. If you can't produce that on demand, your risk-based story has a hole in it.
Step 5: Choose the right tool. The tool should let you target the way you've decided to target, keep a full audit trail, and fit your monitoring model. For teams targeting by time period, Viedoc's EDC platform does this through its SDV Manager application. It's included in the existing license at no extra cost, and keeps a complete record of which plan was active at each site in each period.
Frequently asked questions
What is the difference between TSDV and RBQM? They operate at different levels, so they're complementary rather than rival options. Targeted source data verification (TSDV) is a single practice, verifying selected source data instead of all of it. Risk-based quality management (RBQM) is the wider framework for managing trial quality based on risk. TSDV is one of the verification methods used inside an RBQM approach.
What is targeted SDV in clinical trials? Targeted SDV means verifying a chosen subset of source data against the records, rather than checking every data point. The subset is selected by risk, so monitor time goes where it matters most. You can target by patient or by time period. Regulators accept targeted SDV as part of a risk-based approach.
What is RBQM in clinical trials? Risk-based quality management is a framework for running trial quality around where risk is highest. It typically includes centralized statistical monitoring, key risk indicators (KRIs), quality tolerance limits, and site risk scoring. ICH E6(R3) treats it as a core expectation of good clinical practice. It covers far more than verification alone.
What is the difference between RBM and RBQM? Risk-based monitoring (RBM) is the philosophy of focusing monitoring on the highest-risk sites and data. Risk-based quality management (RBQM) is the broader framework built on that philosophy. RBM tells you where to look. RBQM gives you the full system, with the indicators, the limits, the scoring, and the response. In short, RBM is the idea, and RBQM is the structure around it.
Is 100% SDV still required? No. 100% SDV is not required by the FDA or the EMA. Both accept a risk-based approach, and verifying every data point is now seen as effort spent in the wrong place. ICH E6(R3), finalized in 2025, frames quality management around risk rather than blanket verification. The expectation is a monitoring strategy proportionate to study risk, not a fixed 100% target.
How does the FDA view targeted SDV? The FDA supports it. The FDA's 2013 guidance, Oversight of Clinical Investigations: A Risk-Based Approach to Monitoring, endorses risk-based monitoring and accepts targeted SDV. It expects sponsors to set a monitoring strategy proportionate to study risk, with a documented rationale for what gets verified and why. Targeted SDV is treated as a sound, compliant way to work, not a shortcut.
What does ICH E6(R3) say about SDV? ICH E6(R3), finalized in 2025, makes risk-based quality management a core part of good clinical practice rather than an optional extra. It does not require 100% SDV. Instead, it expects monitoring effort, including SDV, to be directed by risk and supported by a clear rationale. In practice, that endorses targeted SDV: verify the data that carries the most risk, and document why. It is the strongest regulatory signal to date that reducing SDV, done with control, is the expected direction.
Can SDV be safely reduced? Yes, when the reduction is risk-based and documented. The case for reducing SDV is well established. The TransCelerate BioPharma position paper (2013) showed that exhaustive SDV is expensive and adds limited value to data quality, and the CluePoints RBQM industry survey (2023) found that excessive SDV remains common despite the guidance pointing the other way. Safe reduction depends on two things: targeting verification at the data and periods that carry real risk, and being able to show an inspector an active plan and a clean record of what was verified, when, and by whom.
Is targeted SDV part of RBQM? Yes. Targeted SDV is the verification component inside a risk-based approach. RBQM decides where risk concentrates, and targeted SDV is how you verify data efficiently in response. You can run targeted SDV on its own for simpler trials, but you can't run RBQM well while still verifying 100% of data by hand.
Do you need an RBQM platform if your EDC already does targeted SDV? It comes down to what you actually need monitored. A dedicated platform earns its place when you're running statistical monitoring, key risk indicators, and tolerance limits across a large or complex study. If your aim is narrower, keeping verification proportionate to risk, an EDC that handles targeted SDV can stand on its own. Match the tooling to the monitoring you genuinely need, not to the most you could buy.
Patient-based vs time-period-based SDV: which is better? For most trials, time-period-based targeting is the stronger fit. The reason is where risk actually sits. Problems at a site, such as a staffing change or a protocol amendment, hit a stretch of time rather than a set of named patients. Sampling by patient can pass over the exact period when those problems occurred, while period-based targeting points verification straight at it.
Targeted SDV inside the Viedoc EDC platform
Targeted SDV is the verification layer inside a risk-based approach, and Viedoc's EDC platform is built to run that layer well through its SDV Manager application.
It's built straight into Viedoc EDC and included in your existing license at no extra cost. SDV configuration is independent of the study design, so you can manage it across design versions and update plans without CRF version changes. It keeps a complete audit trail of which plan was active at each site in each period, what was verified, when, and by whom. It works for both sponsor and CRO monitoring models, with permission-level visibility. Viedoc EDC is rated 4.5/5 on G2 across 237 reviews.
It does not claim to be a full RBQM platform, and that's the point. It handles the targeted SDV component of your risk-based approach, sitting comfortably alongside whatever monitoring framework you run. If you want to see how time-period targeting works in practice, you can book a demo.
/new-year.jpg)